Biliary Disease
Braden Vogt
Alex Wiles
Pearls
- ERCP is not available at VA: requires fee-basis consult to VUMC, contact GI to arrange
- Prior cholecystectomy -> CBD normally dilates to 10 mm, not pathologic
- Pneuomobilia generally indicates performance of prior biliary sphincterotomy and/or biliary stent
- CBD dilation classically > 6mm, but CBD dilates with age: 70 yo -> 7mm, 80 yo -> 8mm; opiates can also cause biliary dilatation
Acute Calculous Cholecystitis
- Inflammation of the GB from an obstructing stone in the GB neck or cystic duct
- Ddx: PUD, pancreatitis, choledocholithiasis, ascending cholangitis, IBD, Fitz-Hugh Curtis
- Presentation: Severe constant RUQ pain, fever/chills, N/V, + Murphy sign
- Evaluation: CBC (leukocytosis), CMP (mild AST/ALT ↑), Lipase, Lactate, BCx x2
- Imaging: RUQ U/S: gallstones + GB wall thickening or pericholecystic edema
- If U/S non-diagnostic (no stones or GB inflammation)à HIDA Scan (lack of GB filling)
Management: Supportive care, antibiotics, GB drainage
- IVF, correct electrolyte abnormalities, NPO
- Broad spectrum antibiotic coverage
- Place CT-guided procedure consult for cholecystostomy placement vs Endoscopic drainage (transpapillary cystic duct stent via ERCP or cholecystoduodenostomy by EUS)
- Consult EGS if necrosis, perforation, or emphysematous changes present
Management: NPO, IVF, IV Abx until resolved or surgical removal
- Urgent Cholecystectomy (<72H) with EGS;
- If poor surgical candidate: Cholecystostomy with IR; endoscopic drainage options for selected patients (i.e. poor surgical candidates also with ascites)
- Complications: gangrenous cholecystitis, perforation, emphysematous cholecystitis, chole-cysto-enteric fistula, gallstone ileus
Acute Acalculous Cholecystitis
- Inflammation of the GB without obstructing stone (due to stasis and ischemia)
- Presentation: Seen in critically ill/ICU pts; similar history as above; may present as unexplained fever or RUQ mass (rarely jaundice)
- Ddx: calculous cholecystitis, pancreatitis, hepatic abscess
- Evaluation: Same as acute calculous cholecystitis
- Imaging: GB wall thickening, pericholecystic edema, intramural gas, GB distention
Biliary Colic
- Transient biliary obstruction typically at the GB neck without GB inflammation (no fever)
- Presentation: Constant (not colicky) intense, dull RUQ pain and N/V for 30 minutes to 6 hours, then resolves, provoked by fatty foods (CCK), absent Murphy’s sign
- Biliary colic generally consists of discrete episodes separated by weeks to months, and not daily pain
- Evaluation: Normal (CBC, LFTs, Lipase, Lactate) - Imaging: RUQ U/S: cholelithiasis (stones in GB)
- Management: Elective cholecystectomy as outpatient
Choledocholithiasis
Anton de Witte
Braden Vogt
- Obstruction of biliary outflow by CBD stone without inflammation (no fever)
- Impacted cystic duct stone (cholecystitis) with compression of the CBD (Mirizzi syndrome)
- Presentation: RUQ pain (can be painless), N/V and jaundice
- Evaluation: CMP and D-bili (Bili/ALP/ GGT ↑↑↑, AST/ALT mild ↑), CBC (Leukocytosis suggests cholangitis), Lipase
- Imaging: RUQ U/S: dilated CBD (ULN is 6mm) à MRCP/EUS vs ERCP (see below)
- MRCP preferred given non-invasive but has lower sensitivity for smaller stones (consider EUS if still have suspicion despite negative MRCP or if patient contraindication to/intolerance of MRI)
Approach to Choledocholithiasis:
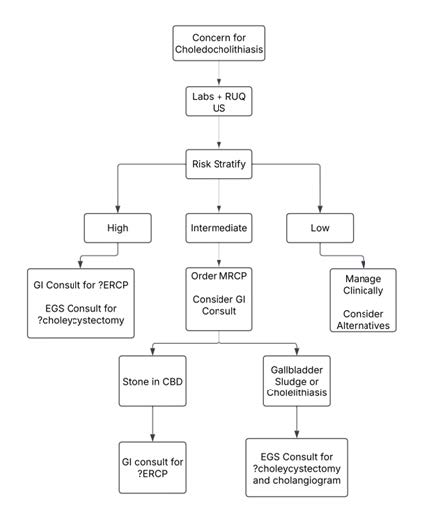
Approach to risk stratification choledocholithiasis:
Risk Profile | Clinical and Imaging Features |
|---|---|
| High | CBD stone on imaging Clinical Acute Cholangitis Tbili > 4 AND dilated CBD (>6mm with GB, > 8mm without GB) |
| Intermediate | Abnormal liver enzymes Age > 55 Dilated CBD on U/S with Tbili < 4 |
| Low | No predictors present |
Management
- NPO & IVF, pain control PRN
- Procedures as per above algorithm
- See Cholangitis section If concern for acute cholangitis
Acute Cholangitis
- Bacterial infection of biliary tract 2/2 obstruction (typically stones) or prior instrumentation (ERCP)
- Pts with malignant obstruction typically do not develop cholangitis
- Presentation: Charcot triad (RUQ pain, fever, jaundice); Reynolds’ Pentad (AMS, Hypotension)
- Evaluation: CBC, CMP (D bili, ALP ↑↑↑) Blood Cultures, Lipase, Lactate o CRP, AST/ALT can be ↑↑ as well
- Imaging: RUQ U/S: dilated CBD (ULN is 6mm), no need for MRCP/EUS
- Consider MRCP overnight if ERCP is not being done emergently
Management
- NPO, IVF
- Consult GI for urgent/emergent ERCP (generally within 24 hr)
- If ERCP not feasible or fails to establish biliary drainage, can consider EUS-guided biliary drainage, percutaneous transhepatic cholangiography, or surgical decompression
- Antibiotics for Biliary Disease (IDSA Guidelines)
- Mild to moderate acute cholecystitis (stable):
- Ceftriaxone 2g daily, Cefazolin 1-2g q8H
- Cholangitis or Severe acute cholecystitis (unstable or immunocompromised):
- Zosyn 3.375g q8H, Meropenem 1g q8H or Cipro 500 q12H and Flagyl 500 q8H
- Healthcare-associated Biliary infections: consider Vancomycin (order w/PK consult)
- Mild to moderate acute cholecystitis (stable):