Definition: acute (hours to days) fluctuating disturbance of attention and awareness due to an underlying medical condition
Complex and multifactorial condition, often due to underlying condition, with unknown pathophysiological mechanisms
Increased morbidity, mortality, and functional decline
Presentation: deficits in attention, orientation, or memory; hallucinations or delusions; sleepwake disturbances; psychomotor changes (hyperactive, hypoactive, or mixed); language impairment; anxious or depressed mood, and/or emotional lability (agitation)
Behavior (hallucinations, restlessness or agitation, psychomotor abnormalities, sleep disturbances)
Cognition (impaired memory, disorientation, disturbances in speech)
Delirium can persist despite identification and reversal of underlying causes, particularly in older patients or those with baseline cognitive deficits.
Evaluation
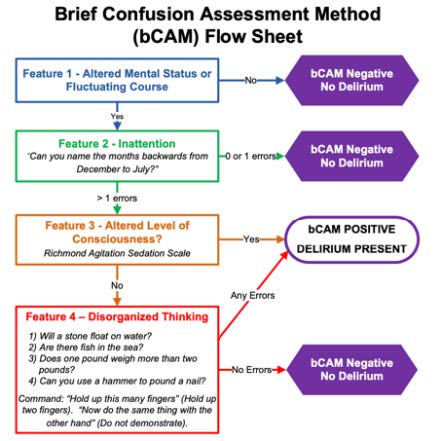
Use screening tools to assess for delirium: Brief Confusion Assessment Method (bCAM). See critical care section for the ICU version, CAM-ICU
Once delirium is diagnosed, evaluate for the underlying cause. Delirium has many etiologies and may occur alone or in combination (in ~10% of cases, no clear cause is found
Mnemonic for common causes of delirium:
D- Drugs/toxins (use of benzodiazepines, opiates, anticholinergics, steroids, etc., withdrawal from ETOH, benzos, etc.)
E- Eyes/ears (sensory deficits)
L- Low perfusion states (MI, PE, heart failure, sepsis)
Are changes needed to address pain control, constipation, insomnia, nausea, etc?
Substance use – evaluate for EtOH or BZD withdrawal state
Empirically load on thiamine (500mg IV tid x9 doses)
EEG – evaluate for seizures, confirm presence of encephalopathic changes
LP – if concerned for CNS infection, inflammatory condition
Management
Treat underlying cause as above
Cognitive impairment or disorientation
Provide clock, calendar, and appropriate lighting
Regular reorientation
Provide cues from a familiar environment (pictures, calls or visits from family members)
Ensure hearing aids, glasses, and dentures are available
Maintain normal sleep-wake cycle
Keep lights on in the day and avoid excessive naps
Early PT, OT interventions, mobilization, move to bedside chair when able
Remove medical support devices as able (foley catheters, restraints, telemetry)
Ensure adequate bowel regimen and hydration
Assess for pain and treat appropriately
Medication reconciliation to reduce or eliminate total anticholinergic load, and to reduce or eliminate other deliriogenic medications as able
See Beers criteria
See critical care section for prevention in the ICU (ABCDEF bundle)
Note on pharmacologic management: There is no pharmacologic intervention known to prevent or treat delirium. Medications for agitation only treat certain behavioral symptoms of delirium, are typically ineffective/harmful for hypoactive delirium, and do not modify the underlying pathological process. Reserve medications for agitation impairing patient safety when non-pharmacologic interventions alone are unsuccessful. See agitation section for medication approach