Basic Chest
X-ray Interpretation
Overview
Always use a systematic approach. It doesn’t matter what the approach is, just be consistent. Below is one example of a search patter.
- Assess quality: AP vs. PA; upright vs. supine; patent positioning; Is the whole chest included?
- Lines/tubes/drains/devices: What lines are present and are they in the expected locations? ET tube, central lines, NG tube/Dobhoff, Pacemaker, valve replacements
- Airway: Is the trachea midline?
- Mediastinum: Is it widened (masses, aortic injury, lymphadenopathy)?
- Cardiac: Is the heart enlarged (cardiothoracic ratio (maximal horizontal cardiac diameter/ maximal horizontal thoracic diameter [inner edge ribs]) on PA CXR should be about 0.4-0.5)
- Pleural space: Is there a pneumothorax? Pleural effusion?
- Rest of image: Look for soft tissue changes—foreign bodies, subcutaneous air. Look for bone abnormalities—fractures, masses. Look for abdominal pathology—air under the diaphragm, position of tubes
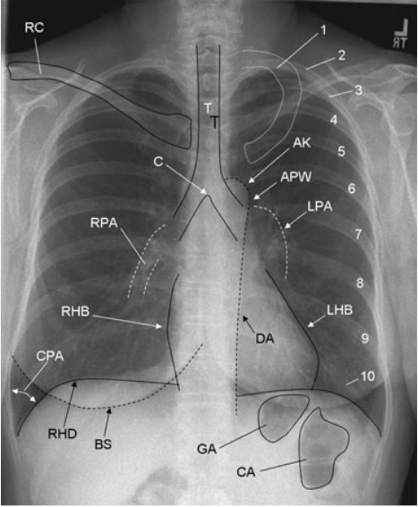
- 1,2-10: first rib, posterior aspect of ribs 2 to 10
- AK: aortic knob
- APW: aortopulmonary window
- BS: breast shadow
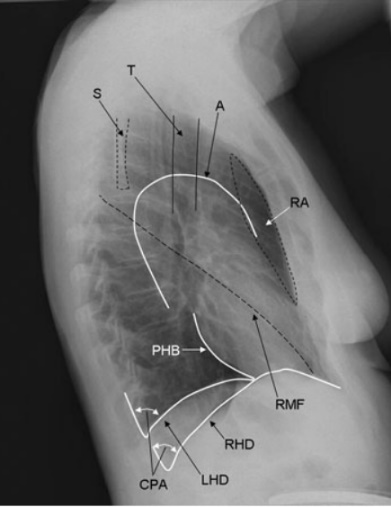
- PHB: posterior heart border
- RHD, LHD: right hemidiaphragm, left hemidiaphragm
- C, T: carina, tracheal air column
- CA, GA: colonic air, gastric air
- CPA: costophrenic angle
- DA: descending aorta
- LHB: left heart border (most of which represents the left ventricle, the superior aspect represents the left atrial appendage)
- RPA: right pulmonary artery
- S: scapula
- RA: retrosternal space
- LPA: left pulmonary artery
- RC: right clavicle
- RHB: right heart border (represents the right atrium)
- RMF: right lung fissure (left major and minor fissures are not always visualized)
Additional resourcees for chest x-ray interpretation
- https://radiologyassistant.nl/chest/chest-x-ray/basic-interpretation
- Felson’s Principles of Chest Roentgenology: a programed text. Available electronically on Eskind Biomedical Library.
- https://radiopaedia.org/articles/chest-radiograph-assessment-using-abcdefghi?lang=us