Basic Abdomen and Pelvis CT Interpretation
Structured search pattern and frequent windowing are important for evaluation of various structures and organs in the abdomen and pelvis.
- Soft tissue window: for evaluation of solid organ and soft tissue structures
- Bone windows: to identify fractures or osseous lesions
- Lung windows: to evaluate lung bases. Also helpful for identifying intraperitoneal free air in the abdomen and pelvis.
Example of routine CT abdomen pelvis search pattern and dictation template:
Lower chest
- Lung bases: consolidation, aspiration, atelectasis
- Pleural effusion, pneumothorax
- Pericardial effusion
Liver
- Assess morphology, enhancement, masses, abscesses, vascular abnormalities, trauma
- Liver trauma: laceration, hematoma, hemorrhage
- Laceration: irregular linear/branching areas of hypoattenuation
- Hematoma: intermediate to hyperdense collection between liver parenchyma and capsule
- Vascular injury
- Active hemorrhage: typically hyperdense compared to normal parenchyma
Gallbladder and biliary tract
- Evaluate for dense gallstones, surrounding fat stranding or fluid, dilated biliary ducts
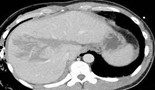
Pancreas
- Assess morphology, enhancement, lesions, ductal dilation, peripancreatic fluid or stranding.
- Pancreatitis: two subtypes (interstitial edematous [seen in image] and necrotizing)
- Parenchymal enlargement, alterations in attenuation, indistinct margins, surrounding fat stranding, lack of parenchymal enhancement suggests necrosis

Spleen
- Size, enhancement, trauma
Adrenal glands
- Morphology, masses
Kidneys and ureters
- Renal size, morphology, enhancement, masses, hydronephrosis, hydroureter, renal or ureteral stones.
- Urolithiasis: distal obstructing ureteral calculus with upstream hydronephrosis
- Pyelonephritis: wedge-like regions of parenchymal swelling and reduced enhancement relative to normal parenchyma

- Complications: renal or perinephric abscess, renal papillary necrosis, emphysematous pyelonephritis (look for bubbly or linear streaks of gas, fluid collections with air-fluid levels)
Urinary bladder
- Not well assessed when decompressed. Assess for wall thickening, masses, intraluminal debris, periserosal fat stranding.
Gastrointestinal tract
- Morphology of distal esophagus and stomach, bowel caliber, wall thickness, masses, mural enhancement, stool burden, appendix
- Bowel obstruction: Dilated gas or fluid-filled loops of bowel (3-6-9 cm rule for upper limit of normal size for small bowel, colon, and cecum diameter), air-fluid levels, fecal matter in small bowel loops, transition point between dilated and collapsed loops of bowel
- Bowel perforation: assess for free air, pneumatosis, portal venous gas
- Pneumatosis intestinalis: Intramural bowel gas. Linear lucencies or rounded bubbly collections.
- Can be life-threatening secondary to ischemia, obstruction, enteritis/colitis, organ transplantation. Can also be incidental and secondary to benign etiology, making clinical context crucial.

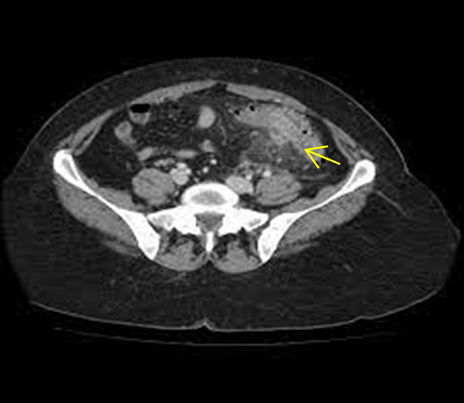
- Diverticulitis: Pericolonic fat stranding, segmental bowel wall thickening, mural hyperenhancement.
- Complicated diverticulitis: perforation (free air and fluid), abscess formation, fistula formation (usually a chronic complication).
- Appendicitis
- Base of appendix located between the ileocecal valve and apex of the cecum.
- Location of the tip of the appendix and length of the appendix are variable.
- Appendiceal dilatation (classically >6mm outer diameter), wall thickening and enhancement, intraluminal fluid, periappendiceal fat stranding, adjacent cecal thickening.
Peritoneum
- Free air, free fluid, fluid collections, peritoneal or omental nodularity/implants
- Small volume of peritoneal fluid may be physiologic in female pts, particularly around menses.
- Fluid is generally hypodense. Hyperdense fluid may suggest hemoperitoneum, especially in context of trauma.
Vasculature
- Suboptimally assessed without intravenous contrast, best assessed with CT angiography
- Portal, splenic, superior mesenteric veins: evaluate patency
- IVC: contrast mixing in IVC can appear similar to a hypodense filling defect.

- Abdominal aorta
- Abdominal aortic aneurysm: focal dilatation >3 cm in maximum transverse diameter.
- Ruptured AAA: retroperitoneal hemorrhage adjacent to aneurysm, blood extending into perirenal or pararenal spaces or psoas muscles. High attenuation crescent representing acute hematoma within mural thrombus or aneurysm wall suggests impending rupture.
- Visceral arteries (celiac, splenic, common hepatic, renal, SMA, IMA)
- Iliac, pelvic, and femoral arteries and veins
Lymph nodes
- Throughout the abdomen and pelvis. Evaluate size (general guideline is <10mm short axis), morphology, enhancement.
- Lower chest, upper abdomen (gastrohepatic ligament, celiac, portocaval, porta hepatis), retroperitoneum, mesentery, pelvis (inguinal, mesorectal, sidewall)
Reproductive organs
- Generally not well evaluated with CT, can be used as an adjunct to imaging with ultrasound or MRI
- Ovarian torsion: enlarged ovary, ovary shifted medially, twisted ovarian pedicle in the adnexa, adnexal fat stranding, underlying ovarian mass.
- Pelvic inflammatory disease: tubular adnexal “mass”, fallopian tube thickening, uterosacral ligament thickening, complex pelvic free fluid, pelvic fat stranding or haziness.
Abdominal wall
- Hernias, hematomas, solid or cystic masses, skin/soft tissue infection
Musculoskeletal
- Important to assess using bone windows
- Fractures
- Destructive osseous lesions
- Degenerative changes
Additional Resources for Abdomen and Pelvis CT Interpretation: